|
||
|
|
||
|
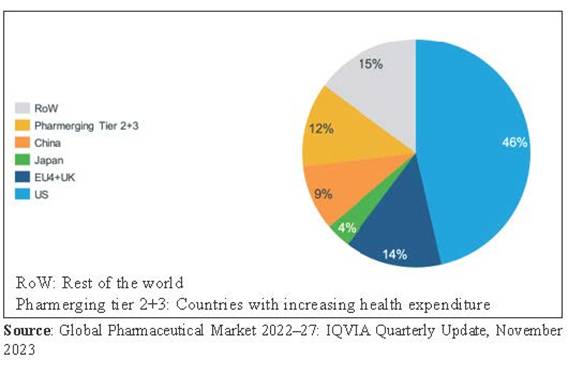
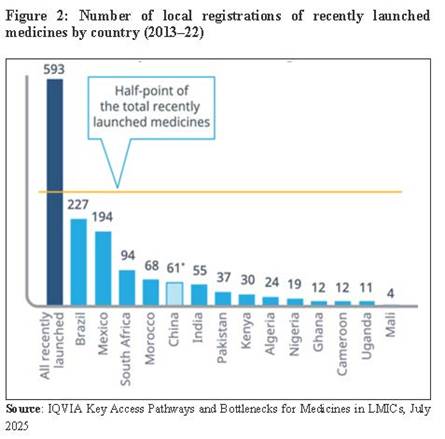
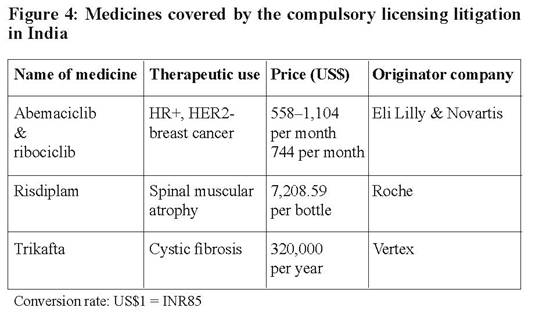
TRIPS@30: Thirty years of widening inequities in access to medicines The TRIPS Agreement, the treaty that sets international standards for the protection of intellectual property, turned 30 this year. In its three decades of implementation, the stringent patenting requirements imposed by the agreement have often thwarted affordable access to medicines in developing countries. K.M. Gopakumar PATENT protection for pharmaceutical products was introduced in developing countries to comply with the World Trade Organization (WTO) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS). As a result, pharmaceutical producers in developing countries lost the freedom to produce generic versions of new medicines. The elimination of freedom of operation has considerably compromised the ability of countries to make available the latest efficacious medicines to the people at affordable prices, widening disparities in access between countries. The COVID-19 pandemic laid bare these contradictions. It not only highlighted the significant inequity in accessing vaccines, therapeutics and diagnostics but also exposed the fallacy of justifying patents as a mechanism to recoup investment in research and development (R&D). Despite the almost 100% public funding, vaccine manufacturers were not ready to license their products widely to facilitate rapid access. Consequently, while high-income countries had vaccinated 68% of their populations by October 2021, only 2.31% of people in low-income countries had received a dose. This is just one of many examples of how a patent is used as a tool to maximise profit at the cost of inequitable access. The United Nations Committee for Development Policy has stated that intellectual property rights �are biased towards rewarding innovators over users. Intellectual property protection often far exceeds what would be necessary to incentivise innovation, leading to high prices and an undersupply of public goods and reducing the global dissemination of the benefits of innovation, which contributes to new inequalities�.1� At the global level, this regime has a clear origin. The 30-year history of the TRIPS Agreement, which came into force in 1995, is a history of institutionalising inequitable access to medicines, barring a few exceptions such as treatments for HIV/AIDS, tuberculosis (TB) and malaria. But even access to new HIV/AIDS and TB therapeutics is threatened by patents. Initiatives to facilitate access, such as the Global Fund to Fight AIDS, TB and Malaria (GFATM) and the US President's Emergency Plan for AIDS Relief (PEPFAR), have been disrupted by the withdrawal of funding from the Trump administration. Meanwhile, a new medicine which can effectively prevent HIV infection has been approved by the US Food and Drug Administration (FDA), bringing with it a possible end to new infections, but patent restrictions could hinder its breakthrough potential. Similarly, more efficacious medicines introduced for the treatment of cancer, rare diseases and other conditions are priced beyond the reach of people in developing countries, largely as a result of patent protections. It is therefore a matter of pressing urgency to examine the options for developing countries in the light of the widening gap in access to medicines. Market concentration The universal introduction of product patent protection by 2005 as required by the TRIPS Agreement, except in least-developed countries (LDCs), helped transnational pharmaceutical corporations to consolidate their market power by eliminating any possibility of competition from generic companies with regard to new medicines. In the absence of competition from generics, the patent holders could charge very high prices in developed countries without the possibility of any comparative pricing. Compulsory product patent protection also allowed the originator companies to obtain patents in developing countries without any obligation to market the product there. After being granted the patents, especially in those developing countries with manufacturing capabilities like China and India, the originator firms could prevent generic manufacturers from producing new medicines. Figure 1 shows the pharmaceutical (excluding vaccines) market distribution among regions. The market is dominated by developed countries: in terms of value, the US, Europe and Japan account for some 64%. This highlights how patent holders have not launched most of the new medicines in developing countries. For the few products which are launched, the high prices make them inaccessible to people and governments in those developing countries. Thus, patent holders can extract the maximum price from developed-country markets through universal pricing (a single price applied globally) and effectively exclude people in developing countries from accessing these patented medicines. Concentration in the vaccine market is even more severe. Ten manufacturers account for 73% of vaccine dose volumes and 85% of global financial value. Manufacturers affiliated with the developing-country vaccine manufacturers� network account for 50% of vaccine doses procured globally, but only 11% of the global financial value. In contrast, manufacturers affiliated with the International Federation of Pharmaceutical Manufacturers & Associations (IFPMA) account for 34% of the volume but 85% of the financial value. On a country basis, high-income countries account for 72% of the financial value of the $77 billion global vaccine market.2 The global spending on medicine in 2024 was at $1.7 trillion, and developed countries accounted for $1.4 trillion.3 The shares of countries with increasing health expenditure (�pharmerging� countries)4 and low-income countries were $312.2 billion and $16.1 billion respectively. Out of the $1,421.5 billion spent in developed countries, $1,091.6 billion was on original brands. The high spending on originator brands is generally due to spending on patented medicines, which are not affordable to the governments and people in developing countries. The high prices emanating from product patent protection have resulted in the denial of access to new medicines in developing countries. According to a report by health analytics firm IQVIA, out of the 1,005 novel active substances (NAS) introduced in the last 20 years, 81% were launched in the US, followed by 65% in Europe and 60% in Japan.5 Though China accounted for 59%, nearly 40% of it was launched only in China. The study does not even mention the percentage of new launches in developing countries. However, citing another IQVIA report, it states that only Brazil and Mexico saw the launch of at least 30% of the most recent NAS (see Figure 2). This clearly shows that originator companies are not launching the majority of their products in many developing countries, which are less attractive from a profitability perspective. The US, Europe and Japan account for 86.8% of the sales of new medicines launched between 2018�23.6 The share of the pharmerging market, which includes China and India, is 3.8%. The rest of the world, including Australia and Canada, accounts for 9.4%. It is clear there is a denial of access to new medicines to people in developing countries. Most patients and governments in these countries are unable to buy these products, irrespective of the actual need. The pharmaceutical market concentration is also reflected in R&D priorities. The pharmaceutical companies focus on the health needs of developed-country markets rather than developing countries. The product patent regime has therefore resulted not only in the denial of access but also in the denial of investment to develop products for diseases disproportionately affecting developing countries. Among those overlooked by this market rationale are the 1.65 million people who require treatment for neglected tropical diseases.7 To make matters worse, over the years, originators have devised various strategies to extend their monopoly beyond the expiry of the original patents: � Product hopping � when an originator slightly modifies a medicine before its patent expires, either by replacing the old version or by promoting the new one, to delay generic competition and extend its market monopoly � Evergreening � when a pharmaceutical company makes minor or incremental changes to a drug, such as a new formulation, dosage, delivery method or combination, often near the end of the patent term, in order to obtain a new patent and extend its market exclusivity without significant therapeutic improvement or actual innovation. In the absence of any legally compulsory measure to market the product at an affordable price in developing countries, the TRIPS Agreement legitimises denial of access to new medicines in the pursuit of intellectual property (IP) protection. It allows originator companies to extract maximum profit from developed-country markets without fear of a comparative generic price. It widens inequity in access and directly compromises the ability of governments, particularly in developing countries, to fulfil their international obligations on the right to health and the right to science. This effectively results in the denial of access to new medicines for the vast majority of people living in developing countries, especially in low- and middle-income countries, where 80% of the world population live. Law and policy response � The standard law and policy response to address concerns emanating from product patent protection is the use of TRIPS flexibilities. The policy flexibilities allowed under the TRIPS Agreement, which are available during the pre- and post-grant stages of patent protection, can be used to facilitate availability of generics at an affordable price. The flexibilities available during the pre-grant stage provide the freedom to set a high threshold for meeting patentability criteria. This can be used to curb the practice of seeking multiple patents on the same molecule and to restrict the number of patents (ideally, one patent per molecule). However, this approach has only had limited success in reining in the practice of extending monopolies. The flexibilities available during the post-grant stage include compulsory and government-use licences to facilitate the production of affordable generic versions of patented products. A government can issue such licences to authorise the production or import of generics without the patent holder�s consent, on the grounds of protecting public health. This policy option can be invoked, for example, during emergencies or when negotiations with the patent holder fail. The patent holder will still receive royalties when such a licence is issued. Another TRIPS flexibility, parallel importing, allows a country to import a patented medicine from another country where it is sold at a lower price, without needing the patent holder�s permission. Though parallel importation is considered an important flexibility, its actual efficacy is doubtful because of the universal pricing policy of originator companies. The use of TRIPS flexibilities to mitigate the adverse effects of product patent protection gained political consensus through the adoption by WTO member states of the Doha Declaration on the TRIPS Agreement and Public Health in 2001. The Declaration affirms that the TRIPS Agreement �can and should be interpreted and implemented in a manner supportive of WTO members' right to protect public health and, in particular, to promote access to medicines for all. In this connection, we reaffirm the right of WTO members to use, to the full, the provisions in the TRIPS Agreement, which provide flexibility for this purpose�. However, countries face many practical challenges in making use of the TRIPS flexibilities, especially compulsory licensing. In the absence of domestic manufacturing capabilities, a country issuing a compulsory licence has to depend on a manufacturer outside its borders to supply the product. Even if producers within the country are able to manufacture a particular pharmaceutical product, they may need to obtain the active pharmaceutical ingredients (API) from elsewhere. Patent protection on the required API could block the supply and therefore render the compulsory licence ineffective.� The TRIPS Agreement was amended in 2017 with a view to facilitating the effective use of compulsory licensing by countries with no domestic manufacturing capacities in the pharmaceutical sector. However, the system put in place under the amendment is riddled with cumbersome procedures and is especially difficult for countries with small markets to utilise, due to lack of economies of scale. As a result of the various challenges, most developing countries cannot use the compulsory licensing option effectively. This is further complicated when voluntary licences are issued by patent holders to generic manufacturers on terms that prevent them from supplying to middle-income countries like Brazil or Malaysia.� In addition, the TRIPS flexibilities are often not fully incorporated into national or regional patent laws. For instance, Figure 3 illustrates the state of implementation of various grounds for compulsory licensing in 114 countries. The table shows that many countries do not explicitly provide grounds for the issuance of a government-use licence. The lack of explicit mention of the grounds could put the countries under undue pressure from patent holders. Further, there may be a lack of institutional and policy measures to make the most of the flexibilities. For example, there is no effective institutional mechanism in most developing countries to monitor the impact of medicine patents on access. As a result, the governments in those countries are not in a position to take timely action to facilitate access to new medicines. Another area where TRIPS flexibilities are seldom utilised is trade secrets. Under Article 39 of the TRIPS Agreement, there is an obligation to keep confidential certain information contained in the dossiers submitted for the marketing approval of medicines. However, an exception to this general rule is provided for in case there is a need to protect the public. This Article allows regulatory authorities to share confidential information to protect public health. However, most countries do not incorporate exceptions to the confidentiality clause for dossiers submitted for marketing approval. Policy space with regard to the use of TRIPS flexibilities is also being circumscribed by free trade agreements (FTAs). FTAs which incorporate �TRIPS-plus� provisions � obligations that go beyond those established in the TRIPS Agreement � eliminate or limit the use of flexibilities. Although some of the new agreements do include language stating that their IP provisions do not affect the freedom to make use of flexibilities, FTAs often contain provisions on providing new-use patents, patent term extensions as well as patent linkage. New-use patents allow companies to extend their monopoly rights by patenting a new use of an existing drug, even when the original patent is about to expire. Patent term extensions prolong a company�s exclusive rights beyond the standard patent period of 20 years, usually to compensate for the time taken for market approval to be granted. Patent linkage ties the drug approval process to patent status, preventing health authorities from approving generic versions until all patents on the originator drug have expired, even if those patents are weak or not directly related. These provisions delay the entry of generic medicines. One of the most important barriers to deploying the TRIPS flexibilities to facilitate access to medicines is bilateral political pressure exerted against their use. Well-documented instances of such pressure led the UN Secretary-General�s High-Level Panel on Access to Medicines to observe that �political and economic pressure placed on governments to forgo the use of TRIPS flexibilities violates the integrity and legitimacy of the system of legal rights and duties created by the TRIPS Agreement, as reaffirmed by the Doha Declaration. This pressure undermines the efforts of states to meet their human rights and public health obligations.�8 � A stark example is the annual �Special 301� report on the global state of IP protection, published by the Office of the US Trade Representative (USTR), the US government agency concerned with trade issues. Countries that make use of TRIPS flexibilities may get listed in the report and be subjected to sanctions by the US. Most recently, the 2025 Special 301 report published under the Trump administration discouraged the use of compulsory licensing, saying that �actions by trading partners to unfairly issue, threaten to issue, or encourage others to issue compulsory licenses raise serious concerns. Such actions can undermine a patent holder�s IP, reduce incentives to invest in research and development for new treatments and cures, unfairly shift the burden for funding such research and development to American patients and those in other markets that properly respect IP ... Such licenses should not be used as a tool to implement industrial policy, including by providing advantages to domestic companies, or as undue leverage in pricing negotiations between governments and right holders�. To evade bilateral political pressure, developing countries like India generally avoid granting compulsory licences and signal their preference for voluntary licences issued by patent holders. However, a voluntary licence not only often excludes middle-income countries but may also impose restrictive conditions to prevent the licensee from supplying to non-licensed territories even under a compulsory licence. The United Nations High Commissioner for Human Rights has noted how this approach undermines equal access to medicines. Seen in this light, voluntary licences are used as a tool to protect profits rather than promote access. Human rights challenges Bilateral political pressures have deterred the issuance of compulsory licences by developing countries. In turn, the inability of developing countries to make optimal use of TRIPS flexibilities compromises their capacity to meet their human rights obligations relating to the right to health and right to science. Further, the TRIPS patent regime in effect leads to discrimination in enjoyment of these rights based on nationality. As shown above, the people in developing countries are denied access to new medicines due to the high prices emanating from product patents. The international human rights framework recognises the adverse implications of the global IP regime, especially with regard to accessing the benefits of scientific research, which include medicines. In its General Comment No. 25 adopted in 2020, the UN Committee on Economic, Social and Cultural Rights (CESCR) highlights how IP is not innate but rather a social product that should be subjected to the rights to health, food and education. However, most national patent laws do not establish any process for patients or patient groups to initiate a compulsory licensing procedure. Therefore, enjoyment of the right to health and the right to science in the context of patented medicines is dependent on the business models of pharmaceutical firms or the discretion of national governments. Left to government discretion, the duty to protect the right to health � which is enshrined in Article 12 of the International Covenant on Economic, Social and Cultural Rights � is seriously undermined. The CESCR�s General Comment No. 14 states that countries must not only be active promoters of the right to health, but also act to guarantee that the right to health is not interfered with by third parties, like private entities. When it comes to private healthcare systems, says the CESCR, the state's intervention is required to guarantee �the availability, accessibility, acceptability and quality of health facilities, goods and services�, and to �control the marketing of medical equipment and medicines by third parties�. However, there are no direct means available within the IP framework, especially in national and regional patent laws, for affected people to remedy the lack of affordable access to patented medicines. At the national level, the administration of patents often falls under the industry or commerce ministry, which may view the use of flexibilities as an option and not a mandatory measure to facilitate access to medicines. Taking note of this situation, the UN Special Rapporteur in the field of cultural rights has stated: �Whereas from the perspective of trade law, exclusions, exceptions and flexibilities under international intellectual property law, such as the World Trade Organization Agreement on Trade-Related Aspects of Intellectual Property Rights, remain optional, from the perspective of human rights, they are often to be considered as obligations.� The optional approach within the IP framework has resulted in the exclusion of individuals or patients from seeking compulsory licences as a remedy against abuse of patent monopolies. Against this backdrop, activists are pushing for realisation of the right to health. In India for example, at least three sets of petitions are pending in two high courts seeking remedy against violation of the fundamental right to health through issuance of government-use licences. These petitions argue that the Indian government has no discretion when it comes to facilitating access to critical patented medicines because lack of access infringes fundamental rights under Article 21 of the Indian Constitution. Article 21 guarantees the right to life, which now extends to the right to live with dignity, including the right to health. Therefore, it is argued, the government should take measures under the country�s Patents Act to facilitate access, like the issuance of a government-use licence. The courts are yet to hear the merits of the petitions and to provide a verdict. Figure 4 gives details of the particular medicines that are the subject of these petitions. Conclusion The TRIPS Agreement, in its three decades of implementation, has entrenched significant inequities in access to medicines, particularly disadvantaging developing countries. While TRIPS flexibilities, such as compulsory licensing, offer legal avenues to mitigate these challenges, practical obstacles, including political pressures, limited manufacturing capacity and cumbersome regulatory frameworks, have severely limited their effectiveness. All these factors have created a chilling effect on the effective use of TRIPS flexibilities. However, the turbulence created by the policies of the Trump administration has once again trained the spotlight on the use of these flexibilities to facilitate affordable access to medicines. The use of flexibilities such as compulsory licensing to remedy abuse of patents offers an effective tool to retaliate against unilateral trade measures unleashed by Washington. Addressing the inequities wrought by medicine patents requires an urgent global commitment to reform the intellectual property regime with a stronger emphasis on public health and human rights obligations. At the same time, there should be renewed efforts to generate the political will to make use of the TRIPS flexibilities to urgently arrest the widening inequity in accessing efficacious medicines and treatments. Towards this end, the international community should actively push back against the political and corporate pressures that undermine the right to health and the right to science. The best way is to empower people individually or collectively with legal remedies against the abuse of patents, such as exorbitant pricing of patented products, by adding appropriate provisions to that effect in patent laws. Only through such comprehensive efforts can the promise of equitable access to medicines and other scientific advances be realised.���� ����������� ������������ K.M. Gopakumar is a senior researcher and legal adviser with the Third World Network. The author acknowledges comments and inputs from Chetali Rao, Rajnia de Vito and Srinath Namboodiri. Notes
Figure 1: Projected pharmaceutical market share (excluding vaccines) between regions (2027)
*Third World Resurgence No. 363, 2025/2, pp 11-16 |
||
|
|
||